Apply to Be a Surrogate With Clear Pay, Protection, and Support
Start your private surrogate application with Yunda. We review your eligibility, answer your questions, and guide you through compensation, screening, legal coordination, insurance review, escrow, and matching.
$61,000+ total compensation package for qualified surrogates
$61,000+ compensation packageIndependent escrow payment protectionLegal and insurance coordinationPrivate review by the Yunda team
I. General Information
ft
in
lbs
Automatically calculated based on height and weight: 0
Occupation or Source of Income *
Marital Status *
Are you a U.S. Citizen or Legal U.S. Resident? *
Ethnicity *
Professionalism. Transparency. Warmth. Protection.
Where Trust Meets Standards
Application overview
What is the Yunda surrogate application?
Surrogacy Requirements (Quick Eligibility)
If you are:
Learn moreyou will receive
Learn moreSurrogacy Process
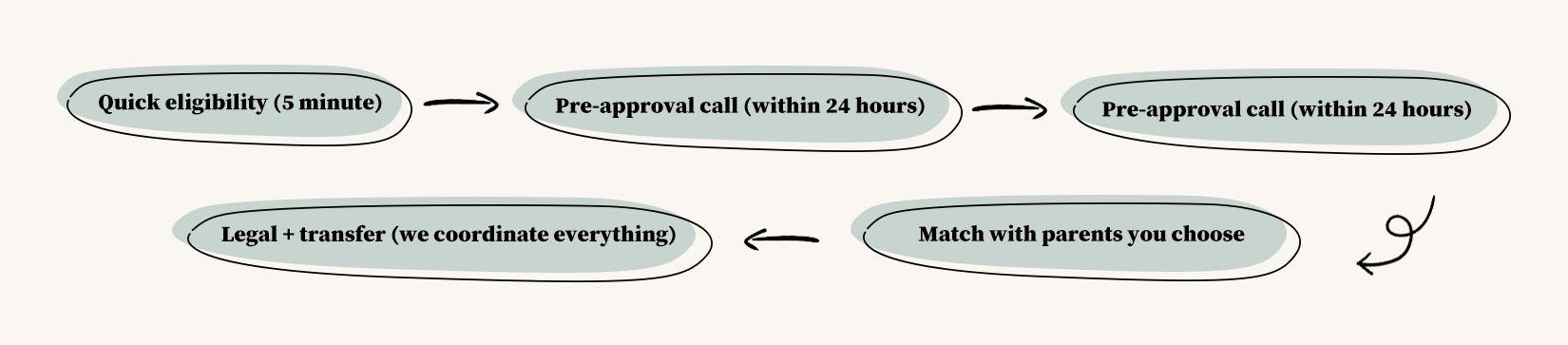
- Quick eligibility (5 minute)
- Pre-approval call (within 24 hours)
- Medical screening (2–4 weeks)
- Match with parents you choose
- Legal + transfer (we coordinate everything)
Protection and support
You should understand your protection before saying yes
Understand the details before you move forward
Questions before applying
Get clear answers before sharing your application
Ready for a private eligibility review?
Our Wonderful Surrogates